
Treatment of Oxidative Stress with Exosomes in Myocardial Ischemia



Department of Cardiovascular Physiology, Graduate School of Medicine, Dentistry, and Pharmaceutical Sciences, Okayama University, Okayama 700-8558, Japan
*
Author to whom correspondence should be addressed.
Int. J. Mol. Sci. 2021, 22(4), 1729; https://doi.org/10.3390/ijms22041729
Submission received: 4 January 2021
/
Revised: 2 February 2021
/
Accepted: 4 February 2021
/
Published: 9 February 2021
(This article belongs to the Special Issue Redox Homeostasis, Signaling, and Oxidative Stress in Health and Disease)
Abstract
:A thrombus in a coronary artery causes ischemia, which eventually leads to myocardial infarction (MI) if not removed. However, removal generates reactive oxygen species (ROS), which causes ischemia–reperfusion (I/R) injury that damages the tissue and exacerbates the resulting MI. The mechanism of I/R injury is currently extensively understood. However, supplementation of exogenous antioxidants is ineffective against oxidative stress (OS). Enhancing the ability of endogenous antioxidants may be a more effective way to treat OS, and exosomes may play a role as targeted carriers. Exosomes are nanosized vesicles wrapped in biofilms which contain various complex RNAs and proteins. They are important intermediate carriers of intercellular communication and material exchange. In recent years, diagnosis and treatment with exosomes in cardiovascular diseases have gained considerable attention. Herein, we review the new findings of exosomes in the regulation of OS in coronary heart disease, discuss the possibility of exosomes as carriers for the targeted regulation of endogenous ROS generation, and compare the advantages of exosome therapy with those of stem-cell therapy. Finally, we explore several miRNAs found in exosomes against OS.
1. Introduction
Cardiovascular disease (CVD) has been the leading cause of mortality in recent years, and its incidence and mortality are closely related to coronary heart disease (CHD). CHD could cause a huge economic burden to regional or national medical systems [1,2]. CHD is, in fact, an inflammatory disease. Oxidative stress (OS) plays an important role in the development of coronary artery disease, and it is mainly caused by an imbalance between reactive oxygen species (ROS) production and endogenous antioxidant defense system. At low levels, ROS causes subtle changes in intracellular pathways, such as redox signal transduction, but at higher levels it causes cell dysfunction and damage [3,4,5]. In the current research on exogenous anti-OS, the effects of OS damage were mot significantly reduced [6,7]. At present, strategies for the clinical treatment and prevention of atherosclerotic CVD still focus on the pharmacotherapy of arachidonic acid metabolism and antiplatelet aggregation (platelet P2Y12 inhibitors), as well as the treatment of related risk factors, such as high blood pressure, excessive lipids, and high blood sugar [8,9,10,11,12,13].
Exosomes are small vesicles [14,15,16] that contain complex RNAs and proteins which are found in natural body fluids, including blood, saliva, urine, cerebrospinal fluid, and milk [17,18]. Discovered in 1946, exosomes were first considered as “clotting factors” [19] that improved coagulation. After 20 years, electron microscopy revealed that platelet products contain vesicles measuring 20–50 nm [20]. Until 1987, Johnstone named these vesicles as “exosomes” [21]. Exosomes can be used as carriers for intercellular communication and can regulate protein expression in receptor cells by RNA transfer [22]. Intercellular communication is necessary in maintaining tissue/organ integrity/homeostasis and inducing adaptive changes to exogenous stimuli. In response to environmental damage and pathological conditions, many cell types release various exosomes of different quality and quantity into the circulation [23,24]. During OS, the exosomes released by cells can mediate signal transduction, change the defense mechanism of receptor cells, and enhance their resistance to OS [23]. In recent years, considerable attention was paid to the important role of exosomes in CVDs, such as ischemic heart disease [25,26,27,28,29].
Exosomes are released from damaged or diseased hearts, playing an important role in disease progression [30,31,32,33]. Considering the related experiments and clinical cell therapy studies, the important roles of exosomes in myocardial injury, repair, and regeneration are being increasingly recognized. According to some studies, the Framingham risk score used to predict CVD risk correlates with circulating exosomes [34,35]. Therefore, exosomes in the circulatory system are potential biomarkers of CVD. The selective packaging of miRNAs in exosomes and their functional transfer through specific signaling molecules are also important for disease treatment [36,37]. In addition, exosomes help detect the endogenous processes of myocardial recovery, regeneration, and protection [38]. They reflect the real-time microenvironment of the lesion, indicating that they are excellent biomarkers in clinical diagnosis. Exosomes are extremely useful because they can determine the pathophysiology of heart disease noninvasively.
In ischemic myocardium, especially after reperfusion, numerous ROS are produced [39,40]. ROS directly damage tissues, inducing cell death. In transgenic mice, infarct size was found to be significantly reduced when the antioxidant protein superoxide dismutase (SOD) was overexpressed [41,42]. Increasing the level of endogenous antioxidants can prevent reperfusion injury [43,44]. Exosomes can provide precise treatment through miRNAs by selecting the corresponding target cells and manipulating the corresponding components; thus, exosomes are a powerful tool for individualized therapy and gene therapy [45,46,47]. Therefore, the upregulation of endogenous antioxidants through exosomes seems to have good prospects. Here, we discuss the potential of exosomes as carriers for regulating endogenous ROS levels to improve the course and prognosis of MI. This work also attempts to discuss the potential of exosomes as biomarkers for CVD. The advantages and disadvantages of exosomes as cell-free therapy are also examined.
2. Exosome-Regulated OS Responses after Myocardial Ischemia
Although initially identified as cell debris, exosomes have many functions regulated by multiple signaling pathways. Exosomes are widely involved in the regulation of OS [48,49] and pathophysiological regulation of various cells; cellular pathophysiological processes include signal transduction, antigen presentation, and immune response [50,51]. Many of the previously conducted studies attempted to provide a detailed summary of the biogenesis of exosomes [52,53,54]. Figure 1 provides an illustration of exosome secretion under OS.
In recent years, many studies concerning CVD highlighted that exosomes not only transport proteins, RNA, DNA, and other molecules under physiological conditions but also participate in pathological conditions such as ischemia–reperfusion (I/R) injury, atherosclerosis, and cardiac remodeling [55,56,57,58,59,60,61]. They can modify gene expression and protein synthesis by inhibiting protein synthesis or initiating mRNA degradation to perform their functions at the post-transcriptional level. Moreover, circulating exosomes are considered as new biomarkers of disease performance and progression [57,62,63].
Under pathological conditions, the exosomes released during OS carry antioxidant molecules, such as superoxide dismutase 1 (SOD1) and glutathione S-transferase (GST) [62,63], and defense molecules, such as glutathione peroxidase 1 (GPX1) [64], which can be absorbed by neighboring cells to enrich their cellular defense mechanisms; thus, these cells are already protected from OS induced by adverse environmental conditions. Therefore, exosomes can potentially transfer defense molecules from one cell to another [65]. For example, in vitro, serum exosomes from healthy human volunteers attenuated H2O2-induced H9c2 cell apoptosis via ERK1/2 signaling pathway activation [66]. Moreover, cardiomyocytes (CMs) secrete miR-30a–rich exosomes after hypoxia stimulation [67]. When the release of miR-30a from exosomes is inhibited, autophagy and OS response in CMs may be maintained after hypoxia [68].
Furthermore, rapid ROS increase and OS occurrence are related to antioxidant depletion. Supplementation of related exogenous antioxidants, such as vitamin E and folic acid, might achieve good effects against OS [69,70]. However, a recent meta-analysis of randomized controlled trials involving 294,478 participants indicated that supplementation of exogenous vitamins and antioxidants was not associated with a reduction in the risk of major CVDs [71]. Interestingly, supplementation with N-acetylcysteine to increase endogenous antioxidants (e.g., glutathione (GSH)) can achieve good antioxidant capacity. After being absorbed by cells, N-acetylcysteine is transformed into cysteine. When the cysteine level increases, the synthesis rate of GSH also increases. More importantly, N-acetylcysteine supplementation not only improves the prognosis of patients but also produces no adverse side effects [72,73,74,75]. Increasing the ratio of GSH/oxidized GSH (GSSG) in patients with heart failure and acute myocardial infarction (MI) can reduce OS and improve the MI area and cardiac function [72,73,74,75]. This finding is also beneficial for the treatment of exosomes, considering that endogenous antioxidants, such as catalase, can be delivered directly through exosomes [76]. Catalase is the main enzyme that regulates H2O2 metabolism. The level of catalase gradually decreases over time after MI [77]. Its overexpression can reduce myocardial I/R injury [78]. After reformation and reshaping of exosomes by sonication and extrusion procedures, catalase could be loaded into exosomes, with a loading capacity of 20–26% [79]. In addition, catalase exosomes can be obtained by modifying parent cells (monocytes/macrophages) and then isolating from the conditioned medium [80].
As natural drug delivery nanoparticles, exosomes have the advantages of cell-based drug delivery and nanoscale size, which aid in achieving effective drug delivery. Exosomes are also lipid vesicles and ideal carriers [81]. In recent years, the application of exosomes as a biomaterial for drug delivery has improved rapidly. At present, treatment with autologous exosomes can help obtain long-term and stable activation of immune effectors [82]. Furthermore, certain drugs can modify exosomes to form carriers with different properties. In mice, the introduction of polyethylene glycol to the exosome surface significantly increased the circulation time of exosomes [83]. However, systemic delivery of exosomes appears to accumulate in the spleen and liver [84,85,86]. To solve this issue, we need to modify the exosomes to increase their targeting to specific tissues or cells. Cells that produce exosomes should be engineered to drive the expression of targeting moieties fused with exosomal membrane proteins. For example, Alvarez-Erviti et al. [87] modified dendritic cells to express Lamp2b, an exosomal membrane protein fused to neuron-specific rabies viral glycoprotein (RVG) peptide, to obtain exosomal targeting. In addition, Wiklander et al. [88] found that compared with unmodified exosomes, RVG-targeted exosomes greatly accumulate in the brain after systemic administration. At the same time, the ability of exosomes to target hypoxic cells in vivo can be enhanced by combining exosomes with hypoxia-targeting peptides or antibodies through bioengineering technology [89,90]. Moreover, exosomes released by different cells, such as immune cells, may be more effective in targeting hypoxic tissue in vivo [91]. An alternative strategy for the noninvasive targeting of magnetic drugs (i.e., enhancing drug delivery to selected tissues by applying a magnetic field gradient) was also proposed decades ago [92,93]. In this strategy, the therapeutic agent and iron oxide nanoparticles together with macrophages are incubated, leading to the production of exosomes loaded with both the therapeutic and magnetic nanoparticles. However, this method may have the disadvantages of toxicity and difficulty in targeting deep tissues. Moreover, exosomes can be used for different ways, such as intraperitoneal injection, subcutaneous injection, and nasal administration. Different administration routes may help improve the therapeutic effect [94]. For example, the intranasal administration of catalase-loaded exosomes in a mouse model of Parkinson’s disease resulted in the increased accumulation of exosomes in brain tissue after four hours [76].
Exosomes as carriers can prevent internal molecular degradation and target special tissues, thereby improving bioavailability and reducing side effects. Moreover, exosomes can serve as carriers for drug delivery and have the potential to easily manipulate the expression of RNA and proteins [87]. Exosomes naturally occur and possess adhesion proteins, which can bind to target cells and remain in target tissues during transplantation [95]. In addition, exosomes have long-term preservation and no degradation because of the existence of resistant membranes. The membrane of exosomes may pass through the blood–brain barrier [96].
Exosomes have great advantages as carriers; however, “nonvesicles,” which are distinct particles that have low electron density without restrictive membranes, are present in exosome preparation [97]. Nonetheless, the appearance of artificial nanovesicles (exosome-mimetic nanovesicles) [91,98] may be helpful in solving this issue.
3. Several Possible Exosomal miRNA Loads
Exosomes contain various molecules, including proteins, lipids, DNA, mRNA, and miRNA, and relevant data can be acquired from the ExoCarta database [99]. Considering the various regulatory roles of miRNA in gene expression, more attention was paid to miRNA. The proportion of miRNA in exosomes is higher than that in their parent cells [100], and miRNA can be transferred between cells through exosomes [22,36]. Meanwhile, miRNAs in exosomes are protected by vesicles and can be stably maintained in circulation; eventually, they are transferred to target cells to inhibit the expression of some genes [101,102]. For example, the knockdown of beta-secretase 1 (BACE1) mRNA and protein was detected in mouse brains after tail vein injection of siRNA-containing exosomes [87]. Therefore, miRNA seems to have a good potential as a content in exosomes.
3.1. MiR-19a
The abnormal expression of miRNA is related to CHD progression. MiR-19a is overexpressed in many cancer types [103,104,105]. However, information about miR-19a in CHD is limited. The plasma miR-19a level in patients with acute MI is significantly higher than that in the control group (up to 120 times), indicating a close relationship between the circulating miR-19a level and sensitivity to acute MI, with this level demonstrating high predictive and distinguishing abilities [106]. After myocardial I/R, apoptosis induced by OS is the key factor of I/R injury. Nevertheless, this damage was significantly reduced by injecting miR-19a into the myocardium of mice after MI [107]. Moreover, miR-19a derived from mesenchymal stem cells (MSC) exosomes could be delivered to the ischemic myocardium to achieve a protective effect [108]. This mechanism is mainly caused by the following ways: 1) miR-19a downregulates the expression of the target proteins in CM, phosphatase and tensin homolog (PTEN), and Bcl-2-like protein 11 (BIM), and activates the Akt and ERK signaling pathways [109]; 2) miR-19a inhibits PTEN in the heart [107,110]. However, this mechanism may not be the only way to protect myocardium. Recently, miR-19a was found to also inhibit OS-induced apoptosis by targeting the three prime untranslated region (3′UTR) of cylindromatosis (CYLD) [111]. Controlled ROS production and nuclear factor kappa-B (NF-κB) inactivation inhibit OS and regulate the expression of miR-19a, thereby inhibiting cell apoptosis induced by OS through the prevention of CYLD proliferation.
3.2. MiR-210
MiR-210 is a miRNA whose expression is induced and regulated by hypoxia, and it also regulates the expression of related genes [112]. MiR-210 has multiple functions because it is upregulated by hypoxia in all tested cell types and tissues [113]. In fact, miR-210 is a target of hypoxia inducible factor-1 (HIF-1) [114]. Under hypoxia, miR-210 regulates multiple cellular processes, such as inhibition of mitochondrial metabolism, promotion of mitochondrial respiration to glycolysis translocation [115], inhibition of apoptosis [116,117], and support in stem-cell survival [118,119].
HIF-1 is a transcription factor that plays an important role in cell response to a hypoxic environment [120]. The HIF-1 activity in the heart is regulated by mRNA changes and HIF-1α protein levels [121,122,123]. On the one hand, HIF-1 can mediate paracrine protection signal in the ischemic heart [124]. This protective effect can not only protect cells in ischemic regions but also potentially improve the survival of transplanted cells [125]. On the other hand, HIF-1 can reduce oxygen consumption by controlling the transcription and post-transcriptional mechanism of cells, that is, cells switch to glycolysis [126]. Under hypoxia, miR-210, which is a known miRNA regulated by HIF-1, is preferentially upregulated by HIF-1 in exosomes. One of the targets of miR-210 is iron–sulfur cluster assembly enzyme (ISCU) [115]. When the ISCU gene is inhibited, the mitochondrial metabolism decreases [125]. The protective effect of HIF-1 and reduced oxygen consumption can reduce ROS production and control the OS level to a certain extent in CMs. Sang-Ging et al. [125] confirmed that transplanted cardiac progenitor cells (CPCs) can resist hypoxia-induced stress in this way. In addition, endothelial cells exposed to hypoxia can produce exosome-rich miR-210 and increase CPC tolerance to OS by stimulating the PI3K/Akt pathway and other survival pathways [127].
3.3. MiR-133a
MiR-133a is one of the most abundant miRNAs in the heart and is crucial in the growth and development of this organ [128,129]. In fact, miR-133a is a biomarker of MI [130]. The serum level of miR-133a is significantly increased in patients with acute MI or unstable angina pectoris [131,132,133] and is closely related to the all-cause mortality rate of patients with acute coronary syndrome [132]. In MI rat models, miR-133 overexpression improved cardiac function through left ventricular ejection fraction and fractional shortening [32].
Furthermore, miR-133a is involved in the early pathology of MI and subsequent cardiac repair [134,135,136]. After hypoxia, the expression of miR-133a was found to change significantly. Overexpression of miR-133a could inhibit hypoxia-induced apoptosis and improve the ability of CMs to resist OS [137,138,139]. In I/R models, miR-133a overexpression significantly reduced CM apoptosis during OS, and this effect is likely to be mediated by targeting death-associated protein kinase 2 (DAPK2) to inhibit I/R injury [140].
MiR-133a also inhibits apoptosis in myocardial ischemic postconditioning, prevents the expression of transgelin 2 (TAGLN2) and caspase-9, and upregulates the expression of antiapoptotic protein Bcl-2 [136,139]. Interestingly, CPC can also benefit from miR-133a by reducing caspase 3 activity and targeting the proapoptotic genes Bim and Bmf [141]. At the same time, miR-133a can improve the anti-OS and survival ability of MSCs by downregulating caspase-9 and Apaf-1 expression [142]. These results indicate the therapeutic value of miR-133a in I/R injury.
4. Advantages of Exosome Therapy in CHD Compared with Those of Stem-Cell Therapy
Over the years, various strategies were tried to find a more effective treatment after CVD occurrence. Currently, stem-cell therapy is an attractive method for CHD prevention and treatment [143,144,145]. In 1993, Koh et al. [146] proved that skeletal muscle myoblasts can be stably transplanted into CMs, demonstrating long-term survival, proliferation, and differentiation. Recently, research focus shifted to bone marrow-derived MSCs [147], and the relevant experiments achieved favorable results [148,149,150]. Previously, differentiation characteristics were the main mechanism for cell transplantation to exert therapeutic effects, however, stem cells did not necessarily differentiate into CMs or endothelial cells after transplantation into ischemic myocardium, but the antiapoptotic, antioxidant stress, and anti-inflammatory effects were mediated by exosomes, thereby improving cardiac function after ischemia [151]. Furthermore, stem-cell transplantation can lead to arrhythmia [152,153,154,155,156,157,158].
The secretory properties of cell transplantation represent an important scientific issue in CHD. Interestingly, exosomes produced during myocardial ischemia can mediate the preventive and therapeutic effects of cell transplantation [159]. Exosomes do have a protective effect on the cardiovascular system [26,160], which was first reported more than 10 years ago [161]. In porcine and mouse models of myocardial I/R injury, 100–200 nm macromolecular complexes secreted by stem cells protected cells under OS. In the subsequent biophysical studies, the biologically active component was characterized as an exosome. More direct evidence suggested that adult stem cells repair heart tissue by releasing paracrine and autocrine factors [162]. For instance, in the isolated Langendorff I/R injury model, purified exosomes derived from MSCs reduced MI in mice [62]. In further experiments, exosome therapy restored the energy consumption and OS levels of the mouse heart within 30 min after I/R and activated cardioprotective PI3K/Akt signaling [163]. Results of a meta-analysis confirmed these cardioprotective effects of MSC-derived exosomes in myocardial injury [164]. I/R results in consumption of intracellular ATP to a large extent, and exosomes from adipose-derived stem cells (ADSCs) were observed to supplement intracellular ATP, NADH, phosphorylated AKT, and phosphorylated GSK-3β levels, while reducing phosphorylated c-JNK and recovering cell bioenergy [165]. The exosomes from ADSCs also increase IL-6 expression and phosphorylate STAT3, which in turn activates the classical signaling pathway and accelerates recovery from injury and angiogenesis after I/R [166]. The effects of exosomes derived from stem cells due to reduction of myocardial OS damage are summarized in Table 1.
Preconditioning can lead to the release of hormones or agonists, such as adenosine [167], opioids [168], and bradykinin [169]. These factors activate related signaling pathways through binding to G protein-coupled receptors, thereby activating PI3K, producing phosphoinositol, and ultimately activating downstream protein kinase B (Akt, also known as PKB or Rac) [170,171]. Davidson et al. provided an overview of exosomes, which mediate the transmission of the cardioprotective signal of remote ischemic preconditioning (RIC) and play a role in reducing OS-mediated damage [172]. Therefore, exosomes have great potential in the treatment of OS caused by MI. Similarly, a group of experiments using cardiac progenitor cell (CPC) exosomes showed that the purified CPC exosomes could be efficiently absorbed by H9c2 cells in vitro and could protect H9c2 from OS by inhibiting caspase 3/7 activation [173]. In Liu et al.’s [66] study, exosomes decreased H9c2 CM apoptosis induced by H2O2, which is the main component of OS, by activating the ERK1/2 signal pathway in vitro, thereby improving the survival rate of H9c2 cells.
Stem cells can be used to treat CVD [177]. Stem-cell therapy is currently being given the utmost research importance, but it possesses some limitations that hinder its widespread use. For example, stem-cell therapy may lead to tumor production [178,179,180]. However, the potential obstacle is their limited survival time in the heart. Implanted MSCs cannot survive for a long time (<1% of MSCs survived after one week of systemic administration) [181,182,183,184]. In the experiment of van Berlo et al., only 0.003% of transplanted cardiac stem cells differentiated into new CMs [185]. Therefore, the ability of repairing myocardial tissue in infarct sites by transplanting stem cells into CMs is limited. Additionally, considerably numerous transplanted MSCs are subsequently embedded in the vascular basement membrane of microvessels and capillaries outside the myocardial tissue [186,187,188]. However, exosomes can target specific tissues and cells through ligand-mediated targeting and magnetic drug targeting. Exosomes can home specific tissues or microenvironments according to their binding molecules. For example, integrins can bind to CMs after myocardial I/R [189] but can also home exosomes to CMs expressing ICAM1, which is a ligand for integrin.
I/R injury is an abnormal reaction of the myocardium after anoxia and reoxygenation. In myocardial I/R injury, cells cannot adapt to the rapid recovery of blood flow and oxygen level after reperfusion, causing various biochemical cascades [190]. Hence, the cells undergo repeated short nonlethal transient I/R cycles to promote biochemical adaptation to reperfusion [191,192,193,194,195]. Exosomes are relatively complex biological entities that contain various molecules, which may provide potential for treating complex injuries such as myocardial I/R injury. Various pathophysiological stress stimuli and disease conditions highly regulate the expression of proteins and RNAs in exosomes [102,196], allowing cells to produce customized exosomes with different functional characteristics. As a result, extensive biochemical and cellular activities occur in the ischemic area to correct the cascade reaction induced by ischemia and hypoxia and to prevent the occurrence of pathological conditions. Exosomes act as intercellular messengers for intercellular communication and aid in exchange of miRNA or proteins [197]. For example, after OS occurs, CPC-derived exosomes load upregulated miR-21 and enter target cells through membrane fusion, thereby inhibiting PDCD4 and cleaved caspase-3 in target cells and reducing cardiomyocyte apoptosis [175]. Moreover, during ischemia and hypoxia, the exosomes of MSC-conditioned medium can significantly reduce the nuclear OS of recipient cells through paracrine mechanisms, thereby reducing apoptosis through reduction of phospho-Smad2 and caspase-3 expression [161]. MiR-93-5p-rich exosomes from ADSCs can target the ATG7 protein through paracrine mechanisms and reduce autophagy and autophagy-related protein expression by targeting Toll-like receptor 4 (TLR4) [174]. Meanwhile, the local microenvironment of the infarct area can affect stem-cell transplantation. For example, the ischemic injury in the infarcted heart hinders the survival of transplanted stem cells, thereby reducing their beneficial effects. Proteins in exosomes secreted by the cells in the infarct area are not affected, but UV treatment can inactivate RNA function in exosomes [23]. Thus, exosome therapy is more effective than stem-cell therapy.
Unlike stem cells, exosomes can maintain their integrity during cryopreservation and transportation because they do not need to be functional. Tumor cell-derived exosomes can mediate drug resistance in chemotherapy and radiotherapy, and drug-resistant cells can transfer drug resistance to target cells through membrane particles in vitro to make these target cells resistant [198], providing cardiac protection for patients during radiotherapy and chemotherapy. At the same time, the exosomes are more stable [199] than stem cells, with no immune rejection [87]. Therefore, exosome-based therapy may be a better option than stem-cell therapy [200].
5. Prospects for the Clinical Application of Exosomes
The new era of the clinical application of exosomes has developed rapidly. In fact, exosomes were approved for use in some clinical trials, and exosome-based therapies are being increasingly applied in humans [201]. Exosomes are robust and stable, making them tremendously attractive as drug delivery tools. Over the past few decades, various methods were invented for loading exosomes with therapeutic drugs, indicating an extension of the drug delivery system. Exosomes may eventually be designed to have a high degree of selectivity and more effective disease targeting. The immunomodulatory and regenerative properties of exosomes are also encouraging for clinical therapy use. Exosomes may replace stem cells in treating OS-induced injury in the cardiovascular system and minimize related concerns and discussions on reducing the tumorigenicity of stem-cell transplantation. Exosome-based therapy was reported to be safe, feasible, and effective in inducing antigen-specific T-lymphocyte responses, but it still has some technical obstacles that must be overcome.
The control of the production and modification of exosomes by parental cells, as well as the quality and function of released exosomes, still require further investigation. Currently, exosomes are characterized by means of size determination and biochemical marker analysis. A more effective protocol to isolate and purify exosomes is also needed to facilitate the vesicles used in clinical research and treatment programs in order to further understand their physiological functions and link their characteristics with pathological results. Although several studies yielded significant findings on exosome therapy, most studies involved in vitro models, making it unclear whether these results reflect in vivo processes. Additionally, most of these studies simply analyzed only a select number of miRNAs or proteins. Studies rarely attempted to investigate all exosomal contents. Therefore, the available results require careful analysis and further studies are warranted in this area. The exosome separation and purification technology suffers from considerable number of limitations and fails to rule out the possibility of protein/lipoprotein contamination [202,203,204]. Moreover, available research suggests that MSCs can release a variety of different subtypes of exosomes [205], which subsequently entails further requirements for the separation and purification of exosomes. At the same time, challenges remain for the reliable tracking of exosomes in vivo, such as the penetration of nanoparticles and magnetic nanoparticles into deep tissues and the toxicity of related nanoparticles. The use of fluorescent lipophilic dyes is not suggested as they are likely to combine with the protein components of the culture medium [206]. Additionally, despite the effectiveness of CDC exosomes after intramyocardial injection, their intracoronary delivery after reperfusion remains ineffective [207]. Therefore, further research is required to elucidate an effective delivery method, such as intravenous injection or a combination of multiple delivery methods.
Currently, the conversion of exosomes to a clinical therapy is limited by the existing regulatory framework, and exosome-based therapy must still be classified. It may be classified into biomedical products or highly advanced therapy medicinal products. Therefore, formulating relevant specific treatment rules may not be necessary. Although relevant documents focusing on regulating exosome-based therapy are available [208], the possibility of requiring more detailed and special rules is not ruled out. For example, identifying, quantifying, and characterizing the main effectors that cause biological effects and determining the mode or mechanism of action may be necessary. However, achieving these tasks may take a long time. According to the existing relevant regulations, several processes still need to be accomplished before using this therapy in clinical trials (e.g., source, immunogenicity, and expected effect) [208,209].
6. Conclusions
Exosomes are involved in various functional behaviors and intercellular communication of cardiac cells, thereby playing an important role in the pathophysiological process of CHD. Given their relevant characteristics, exosomes are considered as therapeutic agents of OS or carriers of related drug therapies. However, the mechanism of OS still requires further exploration, and the application of exosomes into clinical treatment still need time and related experimental tests, which may require support from interdisciplinary research. Once these limitations are solved, exosomes may become a therapeutic tool for CHD.
Author Contributions
Conceptualization, K.T.; investigation, Y.L. (Yun Liu); writing—original draft preparation, Y.L. (Yun Liu); writing—review and editing, M.W., Y.L. (Yin Liang), C.W., K.T.; supervision, K.N.; project administration, K.T.; funding acquisition, K.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Japan Society for the Promotion of Science, grant number 20H04518.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Hao, Y.; Liu, J.; Liu, J.; Yang, N.; Smith, S.C., Jr.; Huo, Y.; Fonarow, G.C.; Ge, J.; Taubert, K.A.; Morgan, L.; et al. Sex differences in in-hospital management and outcomes of patients with acute coronary syndrome. Circulation 2019, 139, 1776–1785. [Google Scholar] [CrossRef]
- Benjamin, E.J.; Muntner, P.; Alonso, A.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Das, S.R.; et al. Heart disease and stroke statistics-2019 update: A report from the american heart association. Circulation 2019, 139, e56–e528. [Google Scholar] [CrossRef]
- Li, R.; Jia, Z.; Trush, M.A. Defining ros in biology and medicine. React. Oxyg. Species 2016, 1, 9–21. [Google Scholar] [CrossRef] [Green Version]
- Angelova, P.R.; Abramov, A.Y. Role of mitochondrial ros in the brain: From physiology to neurodegeneration. FEBS Lett. 2018, 592, 692–702. [Google Scholar] [CrossRef]
- Yang, S.; Lian, G. Ros and diseases: Role in metabolism and energy supply. Mol. Cell. Biochem. 2020, 467, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Lonn, E.; Bosch, J.; Yusuf, S.; Sheridan, P.; Pogue, J.; Arnold, J.M.; Ross, C.; Arnold, A.; Sleight, P.; Probstfield, J.; et al. Effects of long-term vitamin e supplementation on cardiovascular events and cancer: A randomized controlled trial. JAMA 2005, 293, 1338–1347. [Google Scholar] [PubMed] [Green Version]
- van der Pol, A.; van Gilst, W.H.; Voors, A.A.; van der Meer, P. Treating oxidative stress in heart failure: Past, present and future. Eur. J. Heart Fail. 2019, 21, 425–435. [Google Scholar] [CrossRef] [PubMed]
- Weitz, J. Hemostasis, thrombosis, fibrinolysis and cardiovascular disease. In Braunwald’s Heart Disease; Mann, Z., Ed.; Elsevier/Saunders: Philadelphia, PA, USA, 2015; pp. 1809–1833. [Google Scholar]
- Jellinger, P.S.; Handelsman, Y.; Rosenblit, P.D.; Bloomgarden, Z.T.; Fonseca, V.A.; Garber, A.J.; Grunberger, G.; Guerin, C.K.; Bell, D.S.H.; Mechanick, J.I.; et al. American association of clinical endocrinologists and american college of endocrinology guidelines for management of dyslipidemia and prevention of cardiovascular disease. Endocr. Pract. 2017, 23, 1–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kinoshita, M.; Yokote, K.; Arai, H.; Iida, M.; Ishigaki, Y.; Ishibashi, S.; Umemoto, S.; Egusa, G.; Ohmura, H.; Okamura, T.; et al. Japan atherosclerosis society (jas) guidelines for prevention of atherosclerotic cardiovascular diseases 2017. J. Atheroscler. Thromb. 2018, 25, 846–984. [Google Scholar] [CrossRef] [Green Version]
- Grundy, S.M.; Stone, N.J.; Bailey, A.L.; Beam, C.; Birtcher, K.K.; Blumenthal, R.S.; Braun, L.T.; de Ferranti, S.; Faiella-Tommasino, J.; Forman, D.E.; et al. 2018 aha/acc/aacvpr/aapa/abc/acpm/ada/ags/apha/aspc/nla/pcna guideline on the management of blood cholesterol: A report of the american college of cardiology/american heart association task force on clinical practice guidelines. Circulation 2019, 73, e285–e350. [Google Scholar]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E., Jr.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 acc/aha/aapa/abc/acpm/ags/apha/ash/aspc/nma/pcna guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: Executive summary: A report of the american college of cardiology/american heart association task force on clinical practice guidelines. Circulation 2018, 138, e426–e483. [Google Scholar] [CrossRef] [PubMed]
- Ferdinandy, P.; Hausenloy, D.J.; Heusch, G.; Baxter, G.F.; Schulz, R. Interaction of risk factors, comorbidities, and comedications with ischemia/reperfusion injury and cardioprotection by preconditioning, postconditioning, and remote conditioning. Pharmacol. Rev. 2014, 66, 1142–1174. [Google Scholar] [CrossRef] [PubMed]
- Raposo, G.; Stoorvogel, W. Extracellular vesicles: Exosomes, microvesicles, and friends. J. Cell Biol. 2013, 200, 373–383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alenquer, M.; Amorim, M.J. Exosome biogenesis, regulation, and function in viral infection. Viruses 2015, 7, 5066–5083. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doyle, L.M.; Wang, M.Z. Overview of extracellular vesicles, their origin, composition, purpose, and methods for exosome isolation and analysis. Cells 2019, 8, 727. [Google Scholar] [CrossRef] [Green Version]
- Thery, C.; Ostrowski, M.; Segura, E. Membrane vesicles as conveyors of immune responses. Nat. Rev. Immunol. 2009, 9, 581–593. [Google Scholar] [CrossRef]
- van der Pol, E.; Boing, A.N.; Harrison, P.; Sturk, A.; Nieuwland, R. Classification, functions, and clinical relevance of extracellular vesicles. Pharmacol. Rev. 2012, 64, 676–705. [Google Scholar] [CrossRef] [Green Version]
- Chargaff, E.; West, R. The biological significance of the thromboplastic protein of blood. J. Biol. Chem. 1946, 166, 189–197. [Google Scholar] [CrossRef]
- Wolf, P. The nature and significance of platelet products in human plasma. Br. J. Haematol. 1967, 13, 269–288. [Google Scholar] [CrossRef]
- Johnstone, R.M.; Adam, M.; Hammond, J.R.; Orr, L.; Turbide, C. Vesicle formation during reticulocyte maturation. Association of plasma membrane activities with released vesicles (exosomes). J. Biol. Chem. 1987, 262, 9412–9420. [Google Scholar] [CrossRef]
- Valadi, H.; Ekstrom, K.; Bossios, A.; Sjostrand, M.; Lee, J.J.; Lotvall, J.O. Exosome-mediated transfer of mrnas and micrornas is a novel mechanism of genetic exchange between cells. Nat. Cell Biol. 2007, 9, 654–659. [Google Scholar] [CrossRef] [Green Version]
- Eldh, M.; Ekstrom, K.; Valadi, H.; Sjostrand, M.; Olsson, B.; Jernas, M.; Lotvall, J. Exosomes communicate protective messages during oxidative stress; possible role of exosomal shuttle rna. PLoS ONE 2010, 5, e15353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, M.J.; Maghsoudi, T.; Wang, T. Exosomes mediate the intercellular communication after myocardial infarction. Int. J. Med. Sci. 2016, 13, 113–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sluijter, J.P.; Verhage, V.; Deddens, J.C.; van den Akker, F.; Doevendans, P.A. Microvesicles and exosomes for intracardiac communication. Cardiovasc. Res. 2014, 102, 302–311. [Google Scholar] [CrossRef] [Green Version]
- Davidson, S.M.; Takov, K.; Yellon, D.M. Exosomes and cardiovascular protection. Cardiovasc. Drugs Ther. 2017, 31, 77–86. [Google Scholar] [CrossRef] [Green Version]
- Lawson, C.; Vicencio, J.M.; Yellon, D.M.; Davidson, S.M. Microvesicles and exosomes: New players in metabolic and cardiovascular disease. J. Endocrinol. 2016, 228, R57–R71. [Google Scholar] [CrossRef]
- Barile, L.; Moccetti, T.; Marban, E.; Vassalli, G. Roles of exosomes in cardioprotection. Eur. Heart J. 2017, 38, 1372–1379. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, A.; Marban, E. Exosomes: Fundamental biology and roles in cardiovascular physiology. Annu. Rev. Physiol. 2016, 78, 67–83. [Google Scholar] [CrossRef] [Green Version]
- Khan, M.; Nickoloff, E.; Abramova, T.; Johnson, J.; Verma, S.K.; Krishnamurthy, P.; Mackie, A.R.; Vaughan, E.; Garikipati, V.N.; Benedict, C.; et al. Embryonic stem cell-derived exosomes promote endogenous repair mechanisms and enhance cardiac function following myocardial infarction. Circ. Res. 2015, 117, 52–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xie, Z.; Wang, X.; Liu, X.; Du, H.; Sun, C.; Shao, X.; Tian, J.; Gu, X.; Wang, H.; Tian, J.; et al. Adipose-derived exosomes exert proatherogenic effects by regulating macrophage foam cell formation and polarization. J. Am. Heart Assoc. 2018, 7, e007442. [Google Scholar] [CrossRef]
- Chen, Y.; Zhao, Y.; Chen, W.; Xie, L.; Zhao, Z.A.; Yang, J.; Chen, Y.; Lei, W.; Shen, Z. Microrna-133 overexpression promotes the therapeutic efficacy of mesenchymal stem cells on acute myocardial infarction. Stem Cell Res. Ther. 2017, 8, 268. [Google Scholar] [CrossRef]
- Komaki, M.; Numata, Y.; Morioka, C.; Honda, I.; Tooi, M.; Yokoyama, N.; Ayame, H.; Iwasaki, K.; Taki, A.; Oshima, N.; et al. Exosomes of human placenta-derived mesenchymal stem cells stimulate angiogenesis. Stem Cell Res. Ther. 2017, 8, 219. [Google Scholar] [CrossRef]
- Nozaki, T.; Sugiyama, S.; Koga, H.; Sugamura, K.; Ohba, K.; Matsuzawa, Y.; Sumida, H.; Matsui, K.; Jinnouchi, H.; Ogawa, H. Significance of a multiple biomarkers strategy including endothelial dysfunction to improve risk stratification for cardiovascular events in patients at high risk for coronary heart disease. J. Am. Coll. Cardiol. 2009, 54, 601–608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amabile, N.; Cheng, S.; Renard, J.M.; Larson, M.G.; Ghorbani, A.; McCabe, E.; Griffin, G.; Guerin, C.; Ho, J.E.; Shaw, S.Y.; et al. Association of circulating endothelial microparticles with cardiometabolic risk factors in the framingham heart study. Eur. Heart J. 2014, 35, 2972–2979. [Google Scholar] [CrossRef]
- Montecalvo, A.; Larregina, A.T.; Shufesky, W.J.; Stolz, D.B.; Sullivan, M.L.; Karlsson, J.M.; Baty, C.J.; Gibson, G.A.; Erdos, G.; Wang, Z.; et al. Mechanism of transfer of functional micrornas between mouse dendritic cells via exosomes. Blood 2012, 119, 756–766. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stoorvogel, W. Functional transfer of microrna by exosomes. Blood 2012, 119, 646–648. [Google Scholar] [CrossRef]
- Sahoo, S.; Losordo, D.W. Exosomes and cardiac repair after myocardial infarction. Circ. Res. 2014, 114, 333–344. [Google Scholar] [CrossRef]
- Kukielka, G.L.; Smith, C.W.; Manning, A.M.; Youker, K.A.; Michael, L.H.; Entman, M.L. Induction of interleukin-6 synthesis in the myocardium. Potential role in postreperfusion inflammatory injury. Circulation 1995, 92, 1866–1875. [Google Scholar] [CrossRef]
- von Knethen, A.; Callsen, D.; Brune, B. Superoxide attenuates macrophage apoptosis by nf-kappa b and ap-1 activation that promotes cyclooxygenase-2 expression. J. Immunol. 1999, 163, 2858–2866. [Google Scholar] [PubMed]
- Chen, Z.; Siu, B.; Ho, Y.S.; Vincent, R.; Chua, C.C.; Hamdy, R.C.; Chua, B.H. Overexpression of mnsod protects against myocardial ischemia/reperfusion injury in transgenic mice. J. Mol. Cell. Cardiol. 1998, 30, 2281–2289. [Google Scholar] [CrossRef]
- Wang, P.; Chen, H.; Qin, H.; Sankarapandi, S.; Becher, M.W.; Wong, P.C.; Zweier, J.L. Overexpression of human copper, zinc-superoxide dismutase (sod1) prevents postischemic injury. Proc. Natl. Acad. Sci. USA 1998, 95, 4556–4560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suzuki, K.; Murtuza, B.; Sammut, I.A.; Latif, N.; Jayakumar, J.; Smolenski, R.T.; Kaneda, Y.; Sawa, Y.; Matsuda, H.; Yacoub, M.H. Heat shock protein 72 enhances manganese superoxide dismutase activity during myocardial ischemia-reperfusion injury, associated with mitochondrial protection and apoptosis reduction. Circulation 2002, 106, I270–I276. [Google Scholar]
- Peng, X.; Li, Y. Induction of cellular glutathione-linked enzymes and catalase by the unique chemoprotective agent, 3h-1,2-dithiole-3-thione in rat cardiomyocytes affords protection against oxidative cell injury. Pharmacol. Res. 2002, 45, 491–497. [Google Scholar] [CrossRef] [PubMed]
- Nouraee, N.; Mowla, S.J. Mirna therapeutics in cardiovascular diseases: Promises and problems. Front. Genet. 2015, 6, 232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Loughlin, A.J.; Woffindale, C.A.; Wood, M.J. Exosomes and the emerging field of exosome-based gene therapy. Curr. Gene Ther. 2012, 12, 262–274. [Google Scholar] [CrossRef] [PubMed]
- Houseley, J.; LaCava, J.; Tollervey, D. Rna-quality control by the exosome. Nat. Rev. Mol. Cell Biol. 2006, 7, 529–539. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Zheng, Y.; Wang, M.; Yan, M.; Jiang, J.; Li, Z. Exosomes derived mir-126 attenuates oxidative stress and apoptosis from ischemia and reperfusion injury by targeting errfi1. Gene 2019, 690, 75–80. [Google Scholar] [CrossRef]
- Zhang, C.; Wang, J.; Ma, X.; Wang, W.; Zhao, B.; Chen, Y.; Chen, C.; Bihl, J.C. Ace2-epc-exs protect ageing ecs against hypoxia/reoxygenation-induced injury through the mir-18a/nox2/ros pathway. J. Cell. Mol. Med. 2018, 22, 1873–1882. [Google Scholar] [CrossRef]
- Zhang, B.; Yin, Y.; Lai, R.C.; Tan, S.S.; Choo, A.B.; Lim, S.K. Mesenchymal stem cells secrete immunologically active exosomes. Stem Cells Dev. 2014, 23, 1233–1244. [Google Scholar] [CrossRef]
- Zhou, Y.; Xu, H.; Xu, W.; Wang, B.; Wu, H.; Tao, Y.; Zhang, B.; Wang, M.; Mao, F.; Yan, Y.; et al. Exosomes released by human umbilical cord mesenchymal stem cells protect against cisplatin-induced renal oxidative stress and apoptosis in vivo and in vitro. Stem Cell Res. Ther. 2013, 4, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pollet, H.; Conrard, L.; Cloos, A.S.; Tyteca, D. Plasma membrane lipid domains as platforms for vesicle biogenesis and shedding? Biomolecules 2018, 8, 94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gola, A.; Niewolna, M.; Werynska, B. Results of the combined treatment of advanced multiple myeloma by the m-2 protocol: Cyclophosphamide, vincristine, melphalan, nitrosourea and prednisone. Pol. Arch. Med. 1987, 77, 200–205. [Google Scholar]
- Kang, X.; Zuo, Z.; Hong, W.; Tang, H.; Geng, W. Progress of research on exosomes in the protection against ischemic brain injury. Front. Neurosci. 2019, 13, 1149. [Google Scholar] [CrossRef]
- Poe, A.J.; Knowlton, A.A. Exosomes as agents of change in the cardiovascular system. J. Mol. Cell. Cardiol. 2017, 111, 40–50. [Google Scholar] [CrossRef]
- Shanmuganathan, M.; Vughs, J.; Noseda, M.; Emanueli, C. Exosomes: Basic biology and technological advancements suggesting their potential as ischemic heart disease therapeutics. Front. Physiol. 2018, 9, 1159. [Google Scholar] [CrossRef]
- Jansen, F.; Nickenig, G.; Werner, N. Extracellular vesicles in cardiovascular disease: Potential applications in diagnosis, prognosis, and epidemiology. Circ. Res. 2017, 120, 1649–1657. [Google Scholar] [CrossRef] [PubMed]
- Bellin, G.; Gardin, C.; Ferroni, L.; Chachques, J.C.; Rogante, M.; Mitrecic, D.; Ferrari, R.; Zavan, B. Exosome in cardiovascular diseases: A complex world full of hope. Cells 2019, 8, 166. [Google Scholar] [CrossRef] [Green Version]
- Shah, R.; Patel, T.; Freedman, J.E. Circulating extracellular vesicles in human disease. N. Engl. J. Med. 2018, 379, 958–966. [Google Scholar] [CrossRef] [PubMed]
- Hafiane, A.; Daskalopoulou, S.S. Extracellular vesicles characteristics and emerging roles in atherosclerotic cardiovascular disease. Metabolism 2018, 85, 213–222. [Google Scholar] [CrossRef]
- Osteikoetxea, X.; Nemeth, A.; Sodar, B.W.; Vukman, K.V.; Buzas, E.I. Extracellular vesicles in cardiovascular disease: Are they jedi or sith? J. Physiol. 2016, 594, 2881–2894. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, R.C.; Arslan, F.; Lee, M.M.; Sze, N.S.; Choo, A.; Chen, T.S.; Salto-Tellez, M.; Timmers, L.; Lee, C.N.; El Oakley, R.M.; et al. Exosome secreted by msc reduces myocardial ischemia/reperfusion injury. Stem Cell Res. 2010, 4, 214–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fahs, A.; Ramadan, F.; Ghamloush, F.; Ayoub, A.J.; Ahmad, F.A.; Kobeissy, F.; Mechref, Y.; Zhao, J.; Zhu, R.; Hussein, N.; et al. Effects of the oncoprotein pax3-foxo1 on modulation of exosomes function and protein content: Implications on oxidative stress protection and enhanced plasticity. Front. Oncol. 2020, 10, 1784. [Google Scholar] [CrossRef]
- Yan, Y.; Jiang, W.; Tan, Y.; Zou, S.; Zhang, H.; Mao, F.; Gong, A.; Qian, H.; Xu, W. Hucmsc exosome-derived gpx1 is required for the recovery of hepatic oxidant injury. Mol. Ther. 2017, 25, 465–479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saeed-Zidane, M.; Linden, L.; Salilew-Wondim, D.; Held, E.; Neuhoff, C.; Tholen, E.; Hoelker, M.; Schellander, K.; Tesfaye, D. Cellular and exosome mediated molecular defense mechanism in bovine granulosa cells exposed to oxidative stress. PLoS ONE 2017, 12, e0187569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, P.; Liu, Z.; Xie, Y.; Gu, H.; Dai, Q.; Yao, J.; Zhou, L. Serum exosomes attenuate h2o2-induced apoptosis in rat h9c2 cardiomyocytes via erk1/2. J. Cardiovasc. Transl. Res. 2019, 12, 37–44. [Google Scholar] [CrossRef]
- Yang, Y.; Li, Y.; Chen, X.; Cheng, X.; Liao, Y.; Yu, X. Exosomal transfer of mir-30a between cardiomyocytes regulates autophagy after hypoxia. J. Mol. Med. 2016, 94, 711–724. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.Q.; Xu, Y.; Wang, S.H. Effect of exosome-carried mir-30a on myocardial apoptosis in myocardial ischemia-reperfusion injury rats through regulating autophagy. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 7066–7072. [Google Scholar]
- Hamblin, M.; Smith, H.M.; Hill, M.F. Dietary supplementation with vitamin e ameliorates cardiac failure in type i diabetic cardiomyopathy by suppressing myocardial generation of 8-iso-prostaglandin f2alpha and oxidized glutathione. J. Card. Fail. 2007, 13, 884–892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, W.; Tang, R.; Ouyang, S.; Ma, F.; Liu, Z.; Wu, J. Folic acid prevents cardiac dysfunction and reduces myocardial fibrosis in a mouse model of high-fat diet-induced obesity. Nutr. Metab. 2017, 14, 68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Myung, S.K.; Ju, W.; Cho, B.; Oh, S.W.; Park, S.M.; Koo, B.K.; Park, B.J.; Korean Meta-Analysis Study, G. Efficacy of vitamin and antioxidant supplements in prevention of cardiovascular disease: Systematic review and meta-analysis of randomised controlled trials. BMJ 2013, 346, f10. [Google Scholar] [CrossRef] [Green Version]
- Sochman, J.; Vrbska, J.; Musilova, B.; Rocek, M. Infarct size limitation: Acute n-acetylcysteine defense (island trial): Preliminary analysis and report after the first 30 patients. Clin. Cardiol. 1996, 19, 94–100. [Google Scholar] [CrossRef]
- Sochman, J.; Peregrin, J.H. Total recovery of left ventricular function after acute myocardial infarction: Comprehensive therapy with streptokinase, n-acetylcysteine and percutaneous transluminal coronary angioplasty. Int. J. Cardiol. 1992, 35, 116–118. [Google Scholar] [CrossRef]
- Arstall, M.A.; Yang, J.; Stafford, I.; Betts, W.H.; Horowitz, J.D. N-acetylcysteine in combination with nitroglycerin and streptokinase for the treatment of evolving acute myocardial infarction. Safety and biochemical effects. Circulation 1995, 92, 2855–2862. [Google Scholar] [CrossRef] [PubMed]
- Mehra, A.; Shotan, A.; Ostrzega, E.; Hsueh, W.; Vasquez-Johnson, J.; Elkayam, U. Potentiation of isosorbide dinitrate effects with n-acetylcysteine in patients with chronic heart failure. Circulation 1994, 89, 2595–2600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haney, M.J.; Klyachko, N.L.; Zhao, Y.; Gupta, R.; Plotnikova, E.G.; He, Z.; Patel, T.; Piroyan, A.; Sokolsky, M.; Kabanov, A.V.; et al. Exosomes as drug delivery vehicles for parkinson’s disease therapy. J. Control. Release 2015, 207, 18–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khaper, N.; Kaur, K.; Li, T.; Farahmand, F.; Singal, P.K. Antioxidant enzyme gene expression in congestive heart failure following myocardial infarction. Mol. Cell. Biochem. 2003, 251, 9–15. [Google Scholar] [CrossRef]
- Li, G.; Chen, Y.; Saari, J.T.; Kang, Y.J. Catalase-overexpressing transgenic mouse heart is resistant to ischemia-reperfusion injury. Am. J. Physiol. 1997, 273, H1090–H1095. [Google Scholar] [CrossRef]
- Batrakova, E.V.; Kim, M.S. Using exosomes, naturally-equipped nanocarriers, for drug delivery. J. Control. Release 2015, 219, 396–405. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Y.; Haney, M.J.; Gupta, R.; Bohnsack, J.P.; He, Z.; Kabanov, A.V.; Batrakova, E.V. Gdnf-transfected macrophages produce potent neuroprotective effects in parkinson’s disease mouse model. PLoS ONE 2014, 9, e106867. [Google Scholar] [CrossRef]
- van Niel, G.; D’Angelo, G.; Raposo, G. Shedding light on the cell biology of extracellular vesicles. Nat. Rev. Mol. Cell Biol. 2018, 19, 213–228. [Google Scholar] [CrossRef]
- Escudier, B.; Dorval, T.; Chaput, N.; Andre, F.; Caby, M.P.; Novault, S.; Flament, C.; Leboulaire, C.; Borg, C.; Amigorena, S.; et al. Vaccination of metastatic melanoma patients with autologous dendritic cell (dc) derived-exosomes: Results of thefirst phase i clinical trial. J. Transl. Med. 2005, 3, 10. [Google Scholar] [CrossRef] [Green Version]
- Kooijmans, S.A.A.; Fliervoet, L.A.L.; van der Meel, R.; Fens, M.; Heijnen, H.F.G.; van Bergen En Henegouwen, P.M.P.; Vader, P.; Schiffelers, R.M. Pegylated and targeted extracellular vesicles display enhanced cell specificity and circulation time. J. Control. Release 2016, 224, 77–85. [Google Scholar] [CrossRef]
- Imai, T.; Takahashi, Y.; Nishikawa, M.; Kato, K.; Morishita, M.; Yamashita, T.; Matsumoto, A.; Charoenviriyakul, C.; Takakura, Y. Macrophage-dependent clearance of systemically administered b16bl6-derived exosomes from the blood circulation in mice. J. Extracell. Vesicles 2015, 4, 26238. [Google Scholar] [CrossRef] [PubMed]
- Yanez-Mo, M.; Siljander, P.R.; Andreu, Z.; Zavec, A.B.; Borras, F.E.; Buzas, E.I.; Buzas, K.; Casal, E.; Cappello, F.; Carvalho, J.; et al. Biological properties of extracellular vesicles and their physiological functions. J. Extracell Vesicles 2015, 4, 27066. [Google Scholar] [CrossRef] [Green Version]
- Di Rocco, G.; Baldari, S.; Toietta, G. Towards therapeutic delivery of extracellular vesicles: Strategies for in vivo tracking and biodistribution analysis. Stem Cells Int. 2016, 2016, 5029619. [Google Scholar] [CrossRef] [Green Version]
- Alvarez-Erviti, L.; Seow, Y.; Yin, H.; Betts, C.; Lakhal, S.; Wood, M.J. Delivery of sirna to the mouse brain by systemic injection of targeted exosomes. Nat. Biotechnol. 2011, 29, 341–345. [Google Scholar] [CrossRef]
- Wiklander, O.P.; Nordin, J.Z.; O’Loughlin, A.; Gustafsson, Y.; Corso, G.; Mager, I.; Vader, P.; Lee, Y.; Sork, H.; Seow, Y.; et al. Extracellular vesicle in vivo biodistribution is determined by cell source, route of administration and targeting. J. Extracell. Vesicles 2015, 4, 26316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Splith, K.; Bergmann, R.; Pietzsch, J.; Neundorf, I. Specific targeting of hypoxic tumor tissue with nitroimidazole-peptide conjugates. Chem. Med. Chem. 2012, 7, 57–61. [Google Scholar] [CrossRef]
- Lee, K.Y.; Hopkins, J.D.; Syvanen, M. Direct involvement of is26 in an antibiotic resistance operon. J. Bacteriol. 1990, 172, 3229–3236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jang, S.C.; Kim, O.Y.; Yoon, C.M.; Choi, D.S.; Roh, T.Y.; Park, J.; Nilsson, J.; Lotvall, J.; Kim, Y.K.; Gho, Y.S. Bioinspired exosome-mimetic nanovesicles for targeted delivery of chemotherapeutics to malignant tumors. ACS Nano 2013, 7, 7698–7710. [Google Scholar] [CrossRef]
- Widder, K.J.; Senyei, A.E.; Ranney, D.F. Magnetically responsive microspheres and other carriers for the biophysical targeting of antitumor agents. Adv. Pharmacol. Chemother. 1979, 16, 213–271. [Google Scholar] [CrossRef]
- Senyei, A.E.; Reich, S.D.; Gonczy, C.; Widder, K.J. In vivo kinetics of magnetically targeted low-dose doxorubicin. J. Pharm. Sci. 1981, 70, 389–391. [Google Scholar] [CrossRef] [PubMed]
- Vader, P.; Mol, E.A.; Pasterkamp, G.; Schiffelers, R.M. Extracellular vesicles for drug delivery. Adv. Drug Deliv. Rev. 2016, 106, 148–156. [Google Scholar] [CrossRef]
- Carrasco-Ramirez, P.; Greening, D.W.; Andres, G.; Gopal, S.K.; Martin-Villar, E.; Renart, J.; Simpson, R.J.; Quintanilla, M. Podoplanin is a component of extracellular vesicles that reprograms cell-derived exosomal proteins and modulates lymphatic vessel formation. Oncotarget 2016, 7, 16070–16089. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, X.; Xiang, X.; Grizzle, W.; Sun, D.; Zhang, S.; Axtell, R.C.; Ju, S.; Mu, J.; Zhang, L.; Steinman, L.; et al. Treatment of brain inflammatory diseases by delivering exosome encapsulated anti-inflammatory drugs from the nasal region to the brain. Mol. Ther. 2011, 19, 1769–1779. [Google Scholar] [CrossRef] [PubMed]
- Grigor’eva, A.E.; Dyrkheeva, N.S.; Bryzgunova, O.E.; Tamkovich, S.N.; Chelobanov, B.P.; Ryabchikova, E.I. Contamination of exosome preparations, isolated from biological fluids. Biomed. Khim. 2017, 63, 91–96. [Google Scholar] [CrossRef] [Green Version]
- Lunavat, T.R.; Jang, S.C.; Nilsson, L.; Park, H.T.; Repiska, G.; Lasser, C.; Nilsson, J.A.; Gho, Y.S.; Lotvall, J. Rnai delivery by exosome-mimetic nanovesicles-Implications for targeting c-Myc in cancer. Biomaterials 2016, 102, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Simpson, R.J.; Kalra, H.; Mathivanan, S. Exocarta as a resource for exosomal research. J. Extracell. Vesicles 2012, 1, 1. [Google Scholar] [CrossRef]
- Goldie, B.J.; Dun, M.D.; Lin, M.; Smith, N.D.; Verrills, N.M.; Dayas, C.V.; Cairns, M.J. Activity-associated mirna are packaged in map1b-enriched exosomes released from depolarized neurons. Nucleic Acids Res. 2014, 42, 9195–9208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Liu, D.; Chen, X.; Li, J.; Li, L.; Bian, Z.; Sun, F.; Lu, J.; Yin, Y.; Cai, X.; et al. Secreted monocytic mir-150 enhances targeted endothelial cell migration. Mol. Cell 2010, 39, 133–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Jong, O.G.; Verhaar, M.C.; Chen, Y.; Vader, P.; Gremmels, H.; Posthuma, G.; Schiffelers, R.M.; Gucek, M.; van Balkom, B.W. Cellular stress conditions are reflected in the protein and rna content of endothelial cell-derived exosomes. J. Extracell. Vesicles 2012, 1, 1. [Google Scholar] [CrossRef]
- Feng, Y.; Liu, J.; Kang, Y.; He, Y.; Liang, B.; Yang, P.; Yu, Z. Mir-19a acts as an oncogenic microrna and is up-regulated in bladder cancer. J. Exp. Clin. Cancer Res. 2014, 33, 67. [Google Scholar] [CrossRef] [Green Version]
- Anfossi, S.; Giordano, A.; Gao, H.; Cohen, E.N.; Tin, S.; Wu, Q.; Garza, R.J.; Debeb, B.G.; Alvarez, R.H.; Valero, V.; et al. High serum mir-19a levels are associated with inflammatory breast cancer and are predictive of favorable clinical outcome in patients with metastatic her2+ inflammatory breast cancer. PLoS ONE 2014, 9, e83113. [Google Scholar] [CrossRef]
- Wu, T.Y.; Zhang, T.H.; Qu, L.M.; Feng, J.P.; Tian, L.L.; Zhang, B.H.; Li, D.D.; Sun, Y.N.; Liu, M. Mir-19a is correlated with prognosis and apoptosis of laryngeal squamous cell carcinoma by regulating timp-2 expression. Int. J. Clin. Exp. Pathol. 2014, 7, 56–63. [Google Scholar] [PubMed]
- Zhong, J.; He, Y.; Chen, W.; Shui, X.; Chen, C.; Lei, W. Circulating microrna-19a as a potential novel biomarker for diagnosis of acute myocardial infarction. Int. J. Mol. Sci. 2014, 15, 20355–20364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, F.; Kataoka, M.; Liu, N.; Liang, T.; Huang, Z.P.; Gu, F.; Ding, J.; Liu, J.; Zhang, F.; Ma, Q.; et al. Therapeutic role of mir-19a/19b in cardiac regeneration and protection from myocardial infarction. Nat. Commun. 2019, 10, 1802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, S.; Li, L.; Liu, T.; Jiang, W.; Hu, X. Mir-19a/19b-loaded exosomes in combination with mesenchymal stem cell transplantation in a preclinical model of myocardial infarction. Regen. Med. 2020, 15, 1749–1759. [Google Scholar] [CrossRef]
- Yu, B.; Kim, H.W.; Gong, M.; Wang, J.; Millard, R.W.; Wang, Y.; Ashraf, M.; Xu, M. Exosomes secreted from gata-4 overexpressing mesenchymal stem cells serve as a reservoir of anti-apoptotic micrornas for cardioprotection. Int. J. Cardiol. 2015, 182, 349–360. [Google Scholar] [CrossRef] [Green Version]
- Sun, G.; Lu, Y.; Li, Y.; Mao, J.; Zhang, J.; Jin, Y.; Li, Y.; Sun, Y.; Liu, L.; Li, L. Mir-19a protects cardiomyocytes from hypoxia/reoxygenation-induced apoptosis via pten/pi3k/p-akt pathway. Biosci. Rep. 2017, 37, BSR20170899. [Google Scholar] [CrossRef] [Green Version]
- Hong, J.; Wang, Y.; Hu, B.C.; Xu, L.; Liu, J.Q.; Chen, M.H.; Wang, J.Z.; Han, F.; Zheng, Y.; Chen, X.; et al. Transcriptional downregulation of microrna-19a by ros production and nf-kappab deactivation governs resistance to oxidative stress-initiated apoptosis. Oncotarget 2017, 8, 70967–70981. [Google Scholar] [CrossRef]
- Greco, S.; Gaetano, C.; Martelli, F. Hypoxamir regulation and function in ischemic cardiovascular diseases. Antioxid. Redox. Signal 2014, 21, 1202–1219. [Google Scholar] [CrossRef] [Green Version]
- Glazewski, S.; Kossut, M.; Siucinska, E.; Skangiel-Kramska, J. Cholinergic markers in the plasticity of murine barrel field. Acta Neurobiol. Exp. 1990, 50, 163–172. [Google Scholar]
- Semenza, G.L. Targeting hypoxia-inducible factor 1 to stimulate tissue vascularization. J. Investig. Med. 2016, 64, 361–363. [Google Scholar] [CrossRef] [PubMed]
- Chan, S.Y.; Zhang, Y.Y.; Hemann, C.; Mahoney, C.E.; Zweier, J.L.; Loscalzo, J. Microrna-210 controls mitochondrial metabolism during hypoxia by repressing the iron-sulfur cluster assembly proteins iscu1/2. Cell. Metab. 2009, 10, 273–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaccagnini, G.; Maimone, B.; Di Stefano, V.; Fasanaro, P.; Greco, S.; Perfetti, A.; Capogrossi, M.C.; Gaetano, C.; Martelli, F. Hypoxia-induced mir-210 modulates tissue response to acute peripheral ischemia. Antioxid. Redox. Signal 2014, 21, 1177–1188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fasanaro, P.; D’Alessandra, Y.; Di Stefano, V.; Melchionna, R.; Romani, S.; Pompilio, G.; Capogrossi, M.C.; Martelli, F. Microrna-210 modulates endothelial cell response to hypoxia and inhibits the receptor tyrosine kinase ligand ephrin-a3. J. Biol. Chem. 2008, 283, 15878–15883. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.W.; Haider, H.K.; Jiang, S.; Ashraf, M. Ischemic preconditioning augments survival of stem cells via mir-210 expression by targeting caspase-8-associated protein 2. J. Biol. Chem. 2009, 284, 33161–33168. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.W.; Jiang, S.; Ashraf, M.; Haider, K.H. Stem cell-based delivery of hypoxamir-210 to the infarcted heart: Implications on stem cell survival and preservation of infarcted heart function. J. Mol. Med. 2012, 90, 997–1010. [Google Scholar] [CrossRef] [Green Version]
- Ong, S.G.; Hausenloy, D.J. Hypoxia-inducible factor as a therapeutic target for cardioprotection. Pharmacol. Ther. 2012, 136, 69–81. [Google Scholar] [CrossRef] [PubMed]
- Martin, C.; Yu, A.Y.; Jiang, B.H.; Davis, L.; Kimberly, D.; Hohimer, A.R.; Semenza, G.L. Cardiac hypertrophy in chronically anemic fetal sheep: Increased vascularization is associated with increased myocardial expression of vascular endothelial growth factor and hypoxia-inducible factor 1. Am. J. Obstet Gynecol. 1998, 178, 527–534. [Google Scholar] [CrossRef]
- Lee, S.H.; Wolf, P.L.; Escudero, R.; Deutsch, R.; Jamieson, S.W.; Thistlethwaite, P.A. Early expression of angiogenesis factors in acute myocardial ischemia and infarction. N. Engl. J. Med. 2000, 342, 626–633. [Google Scholar] [CrossRef]
- Jurgensen, J.S.; Rosenberger, C.; Wiesener, M.S.; Warnecke, C.; Horstrup, J.H.; Grafe, M.; Philipp, S.; Griethe, W.; Maxwell, P.H.; Frei, U.; et al. Persistent induction of hif-1alpha and -2alpha in cardiomyocytes and stromal cells of ischemic myocardium. FASEB J. 2004, 18, 1415–1417. [Google Scholar] [CrossRef]
- Huang, M.; Nguyen, P.; Jia, F.; Hu, S.; Gong, Y.; de Almeida, P.E.; Wang, L.; Nag, D.; Kay, M.A.; Giaccia, A.J.; et al. Double knockdown of prolyl hydroxylase and factor-inhibiting hypoxia-inducible factor with nonviral minicircle gene therapy enhances stem cell mobilization and angiogenesis after myocardial infarction. Circulation 2011, 124, S46–S54. [Google Scholar] [CrossRef] [Green Version]
- Ong, S.G.; Lee, W.H.; Huang, M.; Dey, D.; Kodo, K.; Sanchez-Freire, V.; Gold, J.D.; Wu, J.C. Cross talk of combined gene and cell therapy in ischemic heart disease: Role of exosomal microrna transfer. Circulation 2014, 130, S60–S69. [Google Scholar] [CrossRef] [Green Version]
- Choudhry, H.; Harris, A.L. Advances in hypoxia-inducible factor biology. Cell. Metab. 2018, 27, 281–298. [Google Scholar] [CrossRef]
- Huang, X.; Zuo, J. Emerging roles of mir-210 and other non-coding rnas in the hypoxic response. Acta Biochim. Biophys. Sin. 2014, 46, 220–232. [Google Scholar] [CrossRef] [Green Version]
- Liu, N.; Bezprozvannaya, S.; Williams, A.H.; Qi, X.; Richardson, J.A.; Bassel-Duby, R.; Olson, E.N. Microrna-133a regulates cardiomyocyte proliferation and suppresses smooth muscle gene expression in the heart. Genes Dev. 2008, 22, 3242–3254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, H.; Lu, Y.; Li, Z.; Wang, Q. Microrna-133: Expression, function and therapeutic potential in muscle diseases and cancer. Curr. Drug Targets 2014, 15, 817–828. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.; Wang, Q.; You, W.; Chen, M.; Xia, J. Mirnas as biomarkers of myocardial infarction: A meta-analysis. PLoS ONE 2014, 9, e88566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuwabara, Y.; Ono, K.; Horie, T.; Nishi, H.; Nagao, K.; Kinoshita, M.; Watanabe, S.; Baba, O.; Kojima, Y.; Shizuta, S.; et al. Increased microrna-1 and microrna-133a levels in serum of patients with cardiovascular disease indicate myocardial damage. Circ. Cardiovasc. Genet. 2011, 4, 446–454. [Google Scholar] [CrossRef]
- Widera, C.; Gupta, S.K.; Lorenzen, J.M.; Bang, C.; Bauersachs, J.; Bethmann, K.; Kempf, T.; Wollert, K.C.; Thum, T. Diagnostic and prognostic impact of six circulating micrornas in acute coronary syndrome. J. Mol. Cell. Cardiol. 2011, 51, 872–875. [Google Scholar] [CrossRef] [PubMed]
- Gacon, J.; Kablak-Ziembicka, A.; Stepien, E.; Enguita, F.J.; Karch, I.; Derlaga, B.; Zmudka, K.; Przewlocki, T. Decision-making micrornas (mir-124, -133a/b, -34a and -134) in patients with occluded target vessel in acute coronary syndrome. Kardiol. Pol. 2016, 74, 280–288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, B.; Xiao, J.; Ren, A.J.; Zhang, Y.F.; Zhang, H.; Chen, M.; Xie, B.; Gao, X.G.; Wang, Y.W. Role of mir-1 and mir-133a in myocardial ischemic postconditioning. J. Biomed. Sci. 2011, 18, 22. [Google Scholar] [CrossRef] [Green Version]
- Yu, B.T.; Yu, N.; Wang, Y.; Zhang, H.; Wan, K.; Sun, X.; Zhang, C.S. Role of mir-133a in regulating tgf-beta1 signaling pathway in myocardial fibrosis after acute myocardial infarction in rats. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 8588–8597. [Google Scholar]
- Li, M.; Ding, W.; Tariq, M.A.; Chang, W.; Zhang, X.; Xu, W.; Hou, L.; Wang, Y.; Wang, J. A circular transcript of ncx1 gene mediates ischemic myocardial injury by targeting mir-133a-3p. Theranostics 2018, 8, 5855–5869. [Google Scholar] [CrossRef]
- Li, A.Y.; Yang, Q.; Yang, K. Mir-133a mediates the hypoxia-induced apoptosis by inhibiting tagln2 expression in cardiac myocytes. Mol. Cell. Biochem. 2015, 400, 173–181. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Wu, Y.; Li, Y.; Xu, C.; Li, X.; Zhu, D.; Zhang, Y.; Xing, S.; Wang, H.; Zhang, Z.; et al. Tanshinone iia improves mir-133 expression through mapk erk1/2 pathway in hypoxic cardiac myocytes. Cell. Physiol. Biochem. 2012, 30, 843–852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, C.; Hu, Y.; Hou, L.; Ju, J.; Li, X.; Du, N.; Guan, X.; Liu, Z.; Zhang, T.; Qin, W.; et al. Beta-blocker carvedilol protects cardiomyocytes against oxidative stress-induced apoptosis by up-regulating mir-133 expression. J. Mol. Cell. Cardiol. 2014, 75, 111–121. [Google Scholar] [CrossRef]
- Li, S.; Xiao, F.Y.; Shan, P.R.; Su, L.; Chen, D.L.; Ding, J.Y.; Wang, Z.Q. Overexpression of microrna-133a inhibits ischemia-reperfusion-induced cardiomyocyte apoptosis by targeting dapk2. J. Hum. Genet. 2015, 60, 709–716. [Google Scholar] [CrossRef] [Green Version]
- Dakhlallah, D.; Zhang, J.; Yu, L.; Marsh, C.B.; Angelos, M.G.; Khan, M. Microrna-133a engineered mesenchymal stem cells augment cardiac function and cell survival in the infarct heart. J. Cardiovasc. Pharmacol. 2015, 65, 241–251. [Google Scholar] [CrossRef] [Green Version]
- Izarra, A.; Moscoso, I.; Levent, E.; Canon, S.; Cerrada, I.; Diez-Juan, A.; Blanca, V.; Nunez-Gil, I.J.; Valiente, I.; Ruiz-Sauri, A.; et al. Mir-133a enhances the protective capacity of cardiac progenitors cells after myocardial infarction. Stem Cell Rep. 2014, 3, 1029–1042. [Google Scholar] [CrossRef] [PubMed]
- Segers, V.F.; Lee, R.T. Stem-cell therapy for cardiac disease. Nature 2008, 451, 937–942. [Google Scholar] [CrossRef]
- Michler, R.E. Stem cell therapy for heart failure. Methodist Debakey Cardiovasc. J. 2013, 9, 187–194. [Google Scholar] [CrossRef] [Green Version]
- Nagaya, N.; Kangawa, K.; Itoh, T.; Iwase, T.; Murakami, S.; Miyahara, Y.; Fujii, T.; Uematsu, M.; Ohgushi, H.; Yamagishi, M.; et al. Transplantation of mesenchymal stem cells improves cardiac function in a rat model of dilated cardiomyopathy. Circulation 2005, 112, 1128–1135. [Google Scholar] [CrossRef] [Green Version]
- Koh, G.Y.; Klug, M.G.; Soonpaa, M.H.; Field, L.J. Differentiation and long-term survival of c2c12 myoblast grafts in heart. J. Clin. Investig. 1993, 92, 1548–1554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mendicino, M.; Bailey, A.M.; Wonnacott, K.; Puri, R.K.; Bauer, S.R. Msc-based product characterization for clinical trials: An fda perspective. Cell Stem Cell 2014, 14, 141–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lalu, M.M.; Mazzarello, S.; Zlepnig, J.; Dong, Y.Y.R.; Montroy, J.; McIntyre, L.; Devereaux, P.J.; Stewart, D.J.; David Mazer, C.; Barron, C.C.; et al. Safety and efficacy of adult stem cell therapy for acute myocardial infarction and ischemic heart failure (safecell heart): A systematic review and meta-analysis. Stem Cells Transl. Med. 2018, 7, 857–866. [Google Scholar] [CrossRef] [Green Version]
- Huang, P.; Wang, L.; Li, Q.; Xu, J.; Xu, J.; Xiong, Y.; Chen, G.; Qian, H.; Jin, C.; Yu, Y.; et al. Combinatorial treatment of acute myocardial infarction using stem cells and their derived exosomes resulted in improved heart performance. Stem Cell Res. Ther. 2019, 10, 300. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.H.; Cho, J.H.; Lee, Y.H.; Lee, J.H.; Kim, S.S.; Kim, M.Y.; Lee, M.G.; Kang, W.Y.; Lee, K.S.; Ahn, Y.K.; et al. Improvement in left ventricular function with intracoronary mesenchymal stem cell therapy in a patient with anterior wall st-segment elevation myocardial infarction. Cardiovasc. Drugs Ther. 2018, 32, 329–338. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, A.G.; Cheng, K.; Marban, E. Exosomes as critical agents of cardiac regeneration triggered by cell therapy. Stem Cell Rep. 2014, 2, 606–619. [Google Scholar] [CrossRef] [Green Version]
- Chong, J.J.; Yang, X.; Don, C.W.; Minami, E.; Liu, Y.W.; Weyers, J.J.; Mahoney, W.M.; Van Biber, B.; Cook, S.M.; Palpant, N.J.; et al. Human embryonic-stem-cell-derived cardiomyocytes regenerate non-human primate hearts. Nature 2014, 510, 273–277. [Google Scholar] [CrossRef] [PubMed]
- Hartman, M.E.; Dai, D.F.; Laflamme, M.A. Human pluripotent stem cells: Prospects and challenges as a source of cardiomyocytes for in vitro modeling and cell-based cardiac repair. Adv. Drug Deliv. Rev. 2016, 96, 3–17. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.M.; Hartzell, C.; Narlow, M.; Dudley, S.C., Jr. Stem cell-derived cardiomyocytes demonstrate arrhythmic potential. Circulation 2002, 106, 1294–1299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, H.S.; Kim, C.; Mercola, M. Electrophysiological challenges of cell-based myocardial repair. Circulation 2009, 120, 2496–2508. [Google Scholar] [CrossRef]
- Menasche, P.; Hagege, A.A.; Vilquin, J.T.; Desnos, M.; Abergel, E.; Pouzet, B.; Bel, A.; Sarateanu, S.; Scorsin, M.; Schwartz, K.; et al. Autologous skeletal myoblast transplantation for severe postinfarction left ventricular dysfunction. J. Am. Coll. Cardiol. 2003, 41, 1078–1083. [Google Scholar] [CrossRef] [Green Version]
- Smits, P.C.; van Geuns, R.J.; Poldermans, D.; Bountioukos, M.; Onderwater, E.E.; Lee, C.H.; Maat, A.P.; Serruys, P.W. Catheter-based intramyocardial injection of autologous skeletal myoblasts as a primary treatment of ischemic heart failure: Clinical experience with six-month follow-up. J. Am. Coll. Cardiol. 2003, 42, 2063–2069. [Google Scholar] [CrossRef] [Green Version]
- Dib, N.; McCarthy, P.; Campbell, A.; Yeager, M.; Pagani, F.D.; Wright, S.; MacLellan, W.R.; Fonarow, G.; Eisen, H.J.; Michler, R.E.; et al. Feasibility and safety of autologous myoblast transplantation in patients with ischemic cardiomyopathy. Cell Transplant. 2005, 14, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Giricz, Z.; Varga, Z.V.; Baranyai, T.; Sipos, P.; Paloczi, K.; Kittel, A.; Buzas, E.I.; Ferdinandy, P. Cardioprotection by remote ischemic preconditioning of the rat heart is mediated by extracellular vesicles. J. Mol. Cell. Cardiol. 2014, 68, 75–78. [Google Scholar] [CrossRef] [Green Version]
- Yellon, D.M.; Davidson, S.M. Exosomes: Nanoparticles involved in cardioprotection? Circ. Res. 2014, 114, 325–332. [Google Scholar] [CrossRef] [PubMed]
- Timmers, L.; Lim, S.K.; Arslan, F.; Armstrong, J.S.; Hoefer, I.E.; Doevendans, P.A.; Piek, J.J.; El Oakley, R.M.; Choo, A.; Lee, C.N.; et al. Reduction of myocardial infarct size by human mesenchymal stem cell conditioned medium. Stem Cell Res. 2007, 1, 129–137. [Google Scholar] [CrossRef] [Green Version]
- Makridakis, M.; Roubelakis, M.G.; Vlahou, A. Stem cells: Insights into the secretome. Biochim. Biophys. Acta 2013, 1834, 2380–2384. [Google Scholar] [CrossRef] [PubMed]
- Arslan, F.; Lai, R.C.; Smeets, M.B.; Akeroyd, L.; Choo, A.; Aguor, E.N.; Timmers, L.; van Rijen, H.V.; Doevendans, P.A.; Pasterkamp, G.; et al. Mesenchymal stem cell-derived exosomes increase atp levels, decrease oxidative stress and activate pi3k/akt pathway to enhance myocardial viability and prevent adverse remodeling after myocardial ischemia/reperfusion injury. Stem Cell Res. 2013, 10, 301–312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, H.; Xiang, M.; Meng, D.; Sun, N.; Chen, S. Inhibition of myocardial ischemia/reperfusion injury by exosomes secreted from mesenchymal stem cells. Stem Cells Int. 2016, 2016, 4328362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Z.; Xu, Y.; Wan, Y.; Gao, J.; Chu, Y.; Li, J. Exosomes from adipose-derived mesenchymal stem cells prevent cardiomyocyte apoptosis induced by oxidative stress. Cell. Death Discov. 2019, 5, 79. [Google Scholar] [CrossRef] [Green Version]
- Pu, C.M.; Liu, C.W.; Liang, C.J.; Yen, Y.H.; Chen, S.H.; Jiang-Shieh, Y.F.; Chien, C.L.; Chen, Y.C.; Chen, Y.L. Adipose-derived stem cells protect skin flaps against ischemia/reperfusion injury via il-6 expression. J. Investig. Dermatol. 2017, 137, 1353–1362. [Google Scholar] [CrossRef] [Green Version]
- Liu, G.S.; Thornton, J.; Van Winkle, D.M.; Stanley, A.W.; Olsson, R.A.; Downey, J.M. Protection against infarction afforded by preconditioning is mediated by a1 adenosine receptors in rabbit heart. Circulation 1991, 84, 350–356. [Google Scholar] [CrossRef] [Green Version]
- Bell, S.P.; Sack, M.N.; Patel, A.; Opie, L.H.; Yellon, D.M. Delta opioid receptor stimulation mimics ischemic preconditioning in human heart muscle. J. Am. Coll. Cardiol. 2000, 36, 2296–2302. [Google Scholar] [CrossRef] [Green Version]
- Goto, M.; Liu, Y.; Yang, X.M.; Ardell, J.L.; Cohen, M.V.; Downey, J.M. Role of bradykinin in protection of ischemic preconditioning in rabbit hearts. Circ. Res. 1995, 77, 611–621. [Google Scholar] [CrossRef]
- Krieg, T.; Qin, Q.; McIntosh, E.C.; Cohen, M.V.; Downey, J.M. Ach and adenosine activate pi3-kinase in rabbit hearts through transactivation of receptor tyrosine kinases. Am. J. Physiol. Heart Circ. Physiol. 2002, 283, H2322–H2330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naga Prasad, S.V.; Barak, L.S.; Rapacciuolo, A.; Caron, M.G.; Rockman, H.A. Agonist-dependent recruitment of phosphoinositide 3-kinase to the membrane by beta-adrenergic receptor kinase 1. A role in receptor sequestration. J. Biol. Chem. 2001, 276, 18953–18959. [Google Scholar] [CrossRef] [Green Version]
- Davidson, S.M.; Andreadou, I.; Barile, L.; Birnbaum, Y.; Cabrera-Fuentes, H.A.; Cohen, M.V.; Downey, J.M.; Girao, H.; Pagliaro, P.; Penna, C.; et al. Circulating blood cells and extracellular vesicles in acute cardioprotection. Cardiovasc. Res. 2019, 115, 1156–1166. [Google Scholar] [CrossRef]
- Chen, L.; Wang, Y.; Pan, Y.; Zhang, L.; Shen, C.; Qin, G.; Ashraf, M.; Weintraub, N.; Ma, G.; Tang, Y. Cardiac progenitor-derived exosomes protect ischemic myocardium from acute ischemia/reperfusion injury. Biochem. Biophys. Res. Commun. 2013, 431, 566–571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, J.; Jiang, M.; Deng, S.; Lu, J.; Huang, H.; Zhang, Y.; Gong, P.; Shen, X.; Ruan, H.; Jin, M.; et al. Mir-93-5p-containing exosomes treatment attenuates acute myocardial infarction-induced myocardial damage. Mol. Ther. Nucleic Acids 2018, 11, 103–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiao, J.; Pan, Y.; Li, X.H.; Yang, X.Y.; Feng, Y.L.; Tan, H.H.; Jiang, L.; Feng, J.; Yu, X.Y. Cardiac progenitor cell-derived exosomes prevent cardiomyocytes apoptosis through exosomal mir-21 by targeting pdcd4. Cell. Death Dis. 2016, 7, e2277. [Google Scholar] [CrossRef] [Green Version]
- Ni, J.; Liu, X.; Yin, Y.; Zhang, P.; Xu, Y.W.; Liu, Z. Exosomes derived from timp2-modified human umbilical cord mesenchymal stem cells enhance the repair effect in rat model with myocardial infarction possibly by the akt/sfrp2 pathway. Oxid. Med. Cell. Longev. 2019, 2019, 1958941. [Google Scholar] [CrossRef] [PubMed]
- Tzahor, E.; Poss, K.D. Cardiac regeneration strategies: Staying young at heart. Science 2017, 356, 1035–1039. [Google Scholar] [CrossRef] [Green Version]
- Swijnenburg, R.J.; Tanaka, M.; Vogel, H.; Baker, J.; Kofidis, T.; Gunawan, F.; Lebl, D.R.; Caffarelli, A.D.; de Bruin, J.L.; Fedoseyeva, E.V.; et al. Embryonic stem cell immunogenicity increases upon differentiation after transplantation into ischemic myocardium. Circulation 2005, 112, I166–I172. [Google Scholar]
- Riess, P.; Molcanyi, M.; Bentz, K.; Maegele, M.; Simanski, C.; Carlitscheck, C.; Schneider, A.; Hescheler, J.; Bouillon, B.; Schafer, U.; et al. Embryonic stem cell transplantation after experimental traumatic brain injury dramatically improves neurological outcome, but may cause tumors. J. Neurotrauma 2007, 24, 216–225. [Google Scholar] [CrossRef] [Green Version]
- Nelson, T.J.; Ge, Z.D.; Van Orman, J.; Barron, M.; Rudy-Reil, D.; Hacker, T.A.; Misra, R.; Duncan, S.A.; Auchampach, J.A.; Lough, J.W. Improved cardiac function in infarcted mice after treatment with pluripotent embryonic stem cells. Anat. Rec. A Discov. Mol. Cell. Evol. Biol. 2006, 288, 1216–1224. [Google Scholar] [CrossRef] [Green Version]
- Toma, C.; Pittenger, M.F.; Cahill, K.S.; Byrne, B.J.; Kessler, P.D. Human mesenchymal stem cells differentiate to a cardiomyocyte phenotype in the adult murine heart. Circulation 2002, 105, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Lee, R.H.; Pulin, A.A.; Seo, M.J.; Kota, D.J.; Ylostalo, J.; Larson, B.L.; Semprun-Prieto, L.; Delafontaine, P.; Prockop, D.J. Intravenous hmscs improve myocardial infarction in mice because cells embolized in lung are activated to secrete the anti-inflammatory protein tsg-6. Cell Stem Cell 2009, 5, 54–63. [Google Scholar] [CrossRef] [Green Version]
- Parekkadan, B.; Milwid, J.M. Mesenchymal stem cells as therapeutics. Annu. Rev. Biomed. Eng. 2010, 12, 87–117. [Google Scholar] [CrossRef] [Green Version]
- Eggenhofer, E.; Benseler, V.; Kroemer, A.; Popp, F.C.; Geissler, E.K.; Schlitt, H.J.; Baan, C.C.; Dahlke, M.H.; Hoogduijn, M.J. Mesenchymal stem cells are short-lived and do not migrate beyond the lungs after intravenous infusion. Front. Immunol. 2012, 3, 297. [Google Scholar] [CrossRef] [Green Version]
- van Berlo, J.H.; Kanisicak, O.; Maillet, M.; Vagnozzi, R.J.; Karch, J.; Lin, S.C.; Middleton, R.C.; Marban, E.; Molkentin, J.D. C-kit+ cells minimally contribute cardiomyocytes to the heart. Nature 2014, 509, 337–341. [Google Scholar] [CrossRef]
- Karp, J.M.; Leng Teo, G.S. Mesenchymal stem cell homing: The devil is in the details. Cell Stem Cell 2009, 4, 206–216. [Google Scholar] [CrossRef] [Green Version]
- Crisan, M.; Yap, S.; Casteilla, L.; Chen, C.W.; Corselli, M.; Park, T.S.; Andriolo, G.; Sun, B.; Zheng, B.; Zhang, L.; et al. A perivascular origin for mesenchymal stem cells in multiple human organs. Cell Stem Cell 2008, 3, 301–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- da Silva Meirelles, L.; Caplan, A.I.; Nardi, N.B. In search of the in vivo identity of mesenchymal stem cells. Stem Cells 2008, 26, 2287–2299. [Google Scholar] [CrossRef] [Green Version]
- Kukielka, G.L.; Hawkins, H.K.; Michael, L.; Manning, A.M.; Youker, K.; Lane, C.; Entman, M.L.; Smith, C.W.; Anderson, D.C. Regulation of intercellular adhesion molecule-1 (icam-1) in ischemic and reperfused canine myocardium. J. Clin. Investig. 1993, 92, 1504–1516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zucchi, R.; Ghelardoni, S.; Evangelista, S. Biochemical basis of ischemic heart injury and of cardioprotective interventions. Curr. Med. Chem. 2007, 14, 1619–1637. [Google Scholar] [CrossRef] [PubMed]
- Na, H.S.; Kim, Y.I.; Yoon, Y.W.; Han, H.C.; Nahm, S.H.; Hong, S.K. Ventricular premature beat-driven intermittent restoration of coronary blood flow reduces the incidence of reperfusion-induced ventricular fibrillation in a cat model of regional ischemia. Am. Heart J. 1996, 132, 78–83. [Google Scholar] [CrossRef]
- Zhao, Z.Q.; Corvera, J.S.; Halkos, M.E.; Kerendi, F.; Wang, N.P.; Guyton, R.A.; Vinten-Johansen, J. Inhibition of myocardial injury by ischemic postconditioning during reperfusion: Comparison with ischemic preconditioning. Am. J. Physiol. Heart Circ. Physiol. 2003, 285, H579–H588. [Google Scholar] [CrossRef]
- Tsang, A.; Hausenloy, D.J.; Mocanu, M.M.; Yellon, D.M. Postconditioning: A form of “modified reperfusion” protects the myocardium by activating the phosphatidylinositol 3-kinase-akt pathway. Circ. Res. 2004, 95, 230–232. [Google Scholar] [CrossRef] [Green Version]
- Yang, X.M.; Proctor, J.B.; Cui, L.; Krieg, T.; Downey, J.M.; Cohen, M.V. Multiple, brief coronary occlusions during early reperfusion protect rabbit hearts by targeting cell signaling pathways. J. Am. Coll Cardiol. 2004, 44, 1103–1110. [Google Scholar] [CrossRef] [Green Version]
- Staat, P.; Rioufol, G.; Piot, C.; Cottin, Y.; Cung, T.T.; L’Huillier, I.; Aupetit, J.F.; Bonnefoy, E.; Finet, G.; Andre-Fouet, X.; et al. Postconditioning the human heart. Circulation 2005, 112, 2143–2148. [Google Scholar] [CrossRef] [PubMed]
- Villarroya-Beltri, C.; Baixauli, F.; Gutierrez-Vazquez, C.; Sanchez-Madrid, F.; Mittelbrunn, M. Sorting it out: Regulation of exosome loading. Semin. Cancer Biol. 2014, 28, 3–13. [Google Scholar] [CrossRef] [Green Version]
- Wortzel, I.; Dror, S.; Kenific, C.M.; Lyden, D. Exosome-mediated metastasis: Communication from a distance. Dev. Cell. 2019, 49, 347–360. [Google Scholar] [CrossRef]
- Bebawy, M.; Combes, V.; Lee, E.; Jaiswal, R.; Gong, J.; Bonhoure, A.; Grau, G.E. Membrane microparticles mediate transfer of p-glycoprotein to drug sensitive cancer cells. Leukemia 2009, 23, 1643–1649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalra, H.; Adda, C.G.; Liem, M.; Ang, C.S.; Mechler, A.; Simpson, R.J.; Hulett, M.D.; Mathivanan, S. Comparative proteomics evaluation of plasma exosome isolation techniques and assessment of the stability of exosomes in normal human blood plasma. Proteomics 2013, 13, 3354–3364. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.; Jiang, C.; Li, R.; Zhao, J. Comparison of endothelial cell- and endothelial progenitor cell-derived exosomes in promoting vascular endothelial cell repair. Int. J. Clin. Exp. Pathol. 2019, 12, 2793–2800. [Google Scholar] [PubMed]
- Mignot, G.; Roux, S.; Thery, C.; Segura, E.; Zitvogel, L. Prospects for exosomes in immunotherapy of cancer. J. Cell. Mol. Med. 2006, 10, 376–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paolini, L.; Zendrini, A.; Di Noto, G.; Busatto, S.; Lottini, E.; Radeghieri, A.; Dossi, A.; Caneschi, A.; Ricotta, D.; Bergese, P. Residual matrix from different separation techniques impacts exosome biological activity. Sci. Rep. 2016, 6, 23550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sodar, B.W.; Kittel, A.; Paloczi, K.; Vukman, K.V.; Osteikoetxea, X.; Szabo-Taylor, K.; Nemeth, A.; Sperlagh, B.; Baranyai, T.; Giricz, Z.; et al. Low-density lipoprotein mimics blood plasma-derived exosomes and microvesicles during isolation and detection. Sci. Rep. 2016, 6, 24316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuana, Y.; Levels, J.; Grootemaat, A.; Sturk, A.; Nieuwland, R. Co-isolation of extracellular vesicles and high-density lipoproteins using density gradient ultracentrifugation. J. Extracell. Vesicles 2014, 3, 23262. [Google Scholar] [CrossRef] [PubMed]
- Lai, R.C.; Tan, S.S.; Yeo, R.W.; Choo, A.B.; Reiner, A.T.; Su, Y.; Shen, Y.; Fu, Z.; Alexander, L.; Sze, S.K.; et al. Msc secretes at least 3 ev types each with a unique permutation of membrane lipid, protein and rna. J. Extracell. Vesicles 2016, 5, 29828. [Google Scholar] [CrossRef]
- Takov, K.; Yellon, D.M.; Davidson, S.M. Confounding factors in vesicle uptake studies using fluorescent lipophilic membrane dyes. J. Extracell. Vesicles 2017, 6, 1388731. [Google Scholar] [CrossRef]
- Gallet, R.; Dawkins, J.; Valle, J.; Simsolo, E.; de Couto, G.; Middleton, R.; Tseliou, E.; Luthringer, D.; Kreke, M.; Smith, R.R.; et al. Exosomes secreted by cardiosphere-derived cells reduce scarring, attenuate adverse remodelling, and improve function in acute and chronic porcine myocardial infarction. Eur. Heart J. 2017, 38, 201–211. [Google Scholar] [CrossRef] [Green Version]
- Lener, T.; Gimona, M.; Aigner, L.; Borger, V.; Buzas, E.; Camussi, G.; Chaput, N.; Chatterjee, D.; Court, F.A.; Del Portillo, H.A.; et al. Applying extracellular vesicles based therapeutics in clinical trials-An isev position paper. J. Extracell. Vesicles 2015, 4, 30087. [Google Scholar] [CrossRef]
- Gedik, N.; Thielmann, M.; Kottenberg, E.; Peters, J.; Jakob, H.; Heusch, G.; Kleinbongard, P. No evidence for activated autophagy in left ventricular myocardium at early reperfusion with protection by remote ischemic preconditioning in patients undergoing coronary artery bypass grafting. PLoS ONE 2014, 9, e96567. [Google Scholar]
Figure 1.
Exosome secretion under OS. Parent cells secrete exosomes containing antioxidant molecules that lead to cardioprotection (A) and/or microRNAs (miRs) that lead to inhibition of apoptosis (B). MSCs secrete SOD1, GPX1, and miR-19a without OS or hypoxia and protect cardiomyocytes exposed to OS. MSC: mesenchymal stem cells; CPC: cardiac progenitor cell; SOD1: superoxide dismutase 1; GPX1: glutathione peroxidase 1; GST: glutathione S-transferase; TAGLN2: transgelin 2; DAPK2: death-associated protein kinase 2; ISCU: iron–sulfur cluster assembly enzyme; PDCD4: programmed cell death 4.
Figure 1.
Exosome secretion under OS. Parent cells secrete exosomes containing antioxidant molecules that lead to cardioprotection (A) and/or microRNAs (miRs) that lead to inhibition of apoptosis (B). MSCs secrete SOD1, GPX1, and miR-19a without OS or hypoxia and protect cardiomyocytes exposed to OS. MSC: mesenchymal stem cells; CPC: cardiac progenitor cell; SOD1: superoxide dismutase 1; GPX1: glutathione peroxidase 1; GST: glutathione S-transferase; TAGLN2: transgelin 2; DAPK2: death-associated protein kinase 2; ISCU: iron–sulfur cluster assembly enzyme; PDCD4: programmed cell death 4.


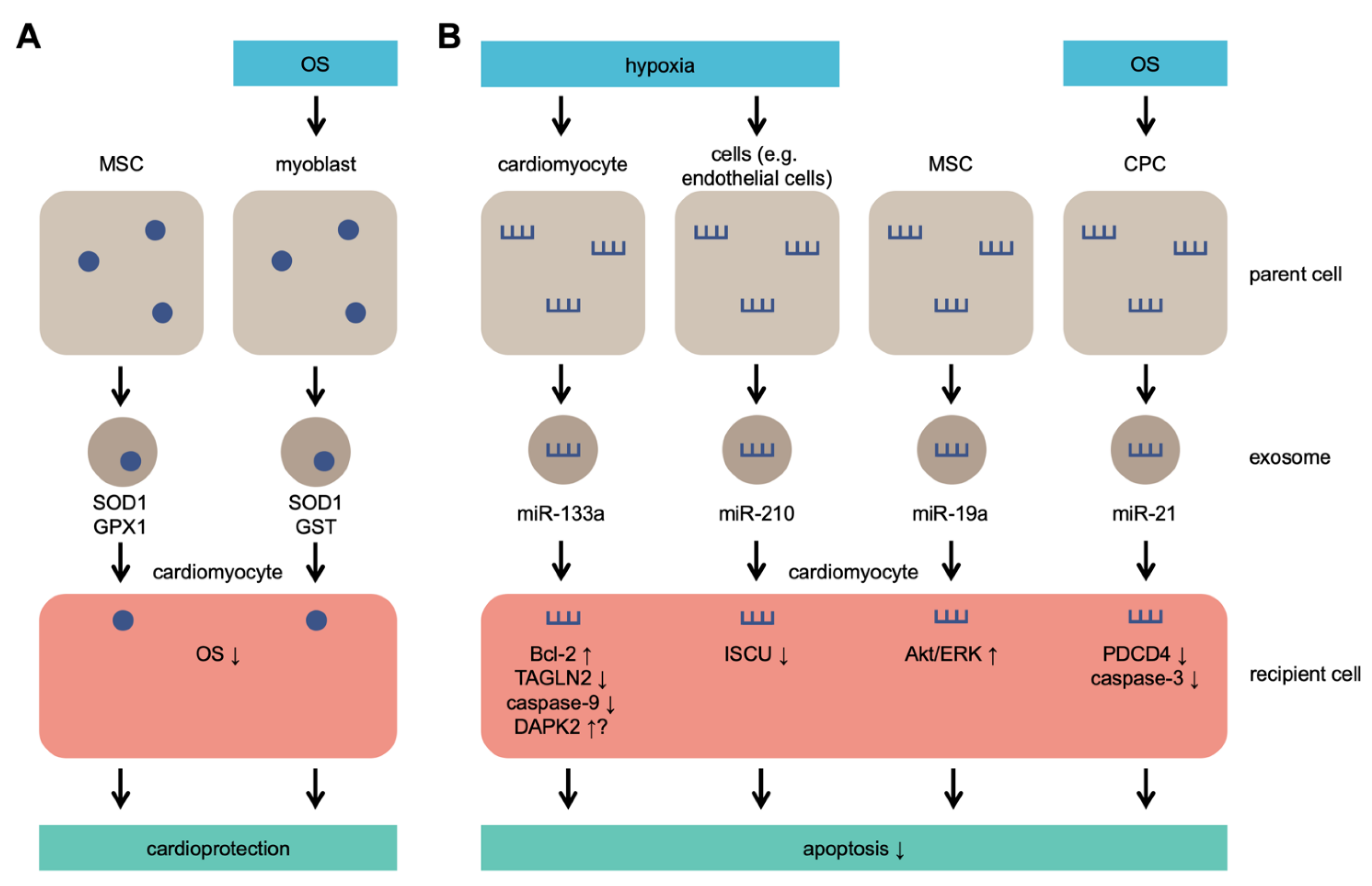{kind=link}
Table 1.
Effect of exosomes derived from stem cells on the reduction of myocardial oxidative stress (OS) damage. ADSC: adipose-derived stem cell; CPC: cardiac progenitor cell; MSC: mesenchymal stem cell; ATG7: autophagy-related 7; TLR4: Toll-like receptor 4; PDCD4: programmed cell death 4.
Table 1.
Effect of exosomes derived from stem cells on the reduction of myocardial oxidative stress (OS) damage. ADSC: adipose-derived stem cell; CPC: cardiac progenitor cell; MSC: mesenchymal stem cell; ATG7: autophagy-related 7; TLR4: Toll-like receptor 4; PDCD4: programmed cell death 4.
| Origin of Exosome | Mechanistic Detail of OS Damage Reduction | References |
|---|---|---|
| ADSC | promotes neovascularization and alleviates inflammation and apoptosis | [165] |
| upregulated miR-93-5p suppresses autophagy and inflammatory cytokine expression by targeting ATG7 and TLR4 | [174] | |
| CPC | upregulated miR-21 inhibits apoptosis by targeting PDCD4 | [175] |
| inhibits caspase 3/7 activity | [173] | |
| activates ERK1/2 pathway and inhibits apoptosis | [66] | |
| MSC | increases ATP level and activates PI3K/Akt pathway | [163] |
| activates Akt/Sfrp2 pathway | [176] | |
| upregulated miR-19a activates Akt/ERK pathway | [109] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Liu, Y.; Wang, M.; Liang, Y.; Wang, C.; Naruse, K.; Takahashi, K. Treatment of Oxidative Stress with Exosomes in Myocardial Ischemia. Int. J. Mol. Sci. 2021, 22, 1729. https://doi.org/10.3390/ijms22041729
AMA Style
Liu Y, Wang M, Liang Y, Wang C, Naruse K, Takahashi K. Treatment of Oxidative Stress with Exosomes in Myocardial Ischemia. International Journal of Molecular Sciences. 2021; 22(4):1729. https://doi.org/10.3390/ijms22041729
Chicago/Turabian StyleLiu, Yun, Mengxue Wang, Yin Liang, Chen Wang, Keiji Naruse, and Ken Takahashi. 2021. "Treatment of Oxidative Stress with Exosomes in Myocardial Ischemia" International Journal of Molecular Sciences 22, no. 4: 1729. https://doi.org/10.3390/ijms22041729
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.